If the COVID vaccine is causing injury and death at an alarming rate, should those not yet vaccinated reconsider getting a COVID shot?
By Nate Dormal | This article was previously published on Stopmandatoryvaccination.com
Vaccine mania is sweeping the nation. One cannot go a day without hearing about the COVID vaccine and the need for increased vaccination rates so “we can get back to normal.” However, since the COVID vaccine supply is now exceeding demand, it reveals that many people do not want the vaccine, and public health authorities are turning to more “coercive” incentives.
Media organizations are pressuring people to get the vaccine by name-calling, universities are requiring the COVID vaccine for those wanting to attend college, criminals are being offered reduced sentences for vaccinating, and businesses are using vaccine passports as an “incentive” to vaccinate despite the public backlash against them and the new inequalities it is creating. All of this occurs in the backdrop of censorship of public health criticism by Big Tech that is implicitly encouraged by lawmakers.
With this new normal, it can feel like we are living in a crazy-land. Even our top politicians have taken a strangely paternalistic obey-us-or-else tone. President Biden tweeted earlier in the week: “The rule is now simple: get vaccinated or wear a mask until you do. The choice is yours.”
All of these efforts have one mission, to “protect” the public from COVID-19. However, an important question remains, “What about COVID vaccine injury & death?”
This simple question should give a pause to all the above efforts as it raises more inconvenient questions. Does it make sense to use coercive measures to drive vaccine uptake when we know that the vaccine will hurt a certain percentage of people? Do freedom and liberty still matter to us in the wake of the pandemic? Do the ends justify the means?
History has shown us that it is easy for us to push aside our critical thinking in the face of crisis. In the drive to deal with terrorism, the Patriot Act infringed upon civil liberties. In the drive to deal with Saddam Hussein’s non-existent “weapons of mass destruction,” over one million Iraqis died due to George W Bush’s War in Iraq.
Now, as we are faced with the COVID crisis, we must not set aside our critical thinking, especially when the costs are measured in American lives and permanent freedoms. We must ask, “What about COVID vaccine injuries and death?”
Is the COVID Vaccine Necessary?
Public health authorities reiterate over the media the message that “if only enough people get the vaccine, then finally we can get back to normal.” But there is a certain hypocrisy to this message for the simple fact that we have heard it before.
We were all told that lockdowns were the answer and that they would be temporary. We were then told that, if only everyone wore masks, that the pandemic would end. As history shows, both of these cases have proven false.
Lockdowns that were justified by the pandemic were proven to be inflated and false. Public health underestimated the costs of the lockdown and the hardships it would impose on the people.
The panacea of widespread masking did not stop the spread of COVID infections. While initially recommended on shaky scientific grounds, the use of masks continued despite problems in studies and failure to find efficacy in randomized controlled trials.
Now we are told that the “only answer” is the COVID vaccine.
There is a pattern here. First, public health authorities zoom onto a single reductionistic solution as The Holy Grail, Second, they utilize force of government to coerce the people into obedience, utilize media and Big Tech to censor criticisms. Third, as later reports emerge of people hurt by their embraced solution, they hide behind their smug “mea culpa” attitude and liability shields.
The answer to the vaccine necessity question lies in what public health and the media isn’t saying.
First, contrary to what they would like you to believe, in actuality, on the whole, we as a populace are very strong. The CDC’s data shows the vast majority of us tolerate and fight off COVID infections. Interestingly enough, the data indicates that the risk of children dying from COVID are akin to being struck by lightning. When over 99.8% survive COVID, the media’s use of fear campaigns to drive vaccine uptake is dishonest.
Second, there are safe and available prophylaxis and treatments for COVID that do not involve the vaccine. The drug ivermectin, as well as a number of nutriceuticals, has been shown to be efficacious in treating COVID.
In their study, the Front Line COVID-19 Critical Care Alliance, demonstrated the efficacy of ivermectin as both a treatment and prophylaxis, and also the the efficacy of their I-MASK+ protocol below:
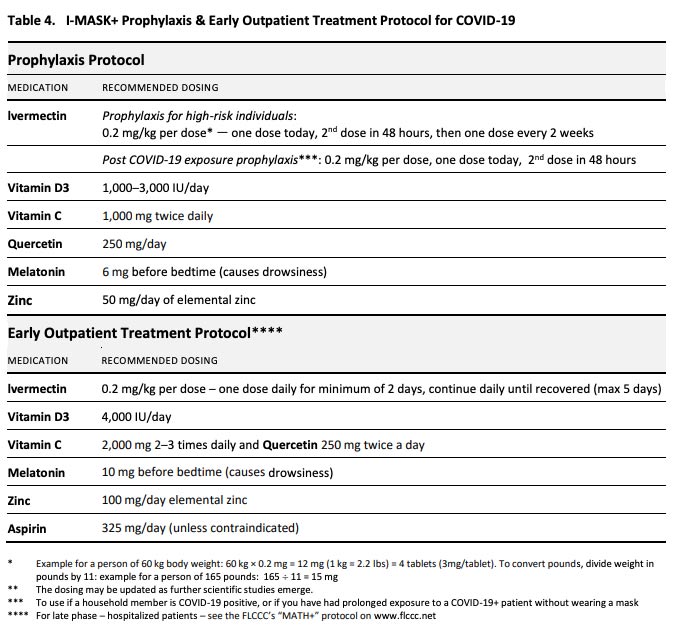
Rather than embrace these alternative treatments, the FDA has instead dismissed and denied their efficacy. As both Yale epidemiologist Harvey Risch and physician Dr. Peter McCullough have argued, the COVID treatment denial is costing needless American lives. So why does the FDA persist in these denials?
People often forget that the COVID vaccines are approved for use under Emergency Use Authorization. The terms for EUA dictate that there can be no viable, alternative treatments for the condition in question.
The above alternatives call into question the FDA EUA for the COVID vaccines. There is already a citizen’s petition campaign to recall the vaccine under these grounds. It also calls into question the authorities’ message that the “only answer is a vaccine.”
Third, the COVID vaccines have not been shown to be effective at preventing transmission of COVID-19. If the COVID vaccine has not been shown to stop transmission, then how can public health demand that citizens take the vaccine to promote “herd immunity”?
According to FDA documents: “Data are limited to assess the effect of the vaccine against transmission of SARS-CoV-2 from individuals who are infected despite vaccination.”
The World Health Organization stated: “We do not know whether the vaccine will prevent infection and protect against onward transmission. Immunity persists for several months, but the full duration is not yet known. These important questions are being studied.”
The fact is that many people, including American political commentator Bill Maher, are still getting positive tests for and getting infected with COVID even after receiving the COVID shot. As of May 17, 2021, the CDC reported that there had been nearly 300 COVID deaths in previously vaccinated individuals.
Finally, the media touts the “95% efficacy” for the COVID vaccine. But it has to be kept in mind that these are relative risk reductions obtained from comparing COVID occurrences between the vaccinated and placebo groups. To ascertain the actual benefits we would have to look at the absolute risk reduction. An AIER article estimates the absolute risk reduction to be only 0.84%.
Rather than ask the blanket question. “Is the COVID vaccine necessary?” you should ask the question, “Is the COVID vaccine necessary for me?”
Ultimately, you are the one bearing the costs of the decision and you, not public health authorities, know your own circumstances the best. Keeping into account the considerations discussed in this article, you should calculate the risk/benefits analysis for yourself
The media seldom acknowledges a very important risk to the vaccination decision – the risk of vaccine injury and death.
Is the COVID Vaccine the Most Dangerous Vaccine Ever?
In a recent show, political commentator Tucker Carlson stated a very crucial fact that should give us pause: “more deaths have been reported from the Covid vaccine in four months than from all other vaccines combined in more than a decade and a half.”
To put these deaths into perspective, Tucker Carlson mentioned another important fact: “In 1976, 45 million Americans were vaccinated for H1N1. A total of 53 people died from the vaccine. The US government halted the vaccination program because authorities decided it was too risky.”
The following graphic (from openVAERS.com) shows the reported deaths and injuries from the COVID vaccine from the US government’s Vaccine Adverse Effects Reporting System (VAERS):
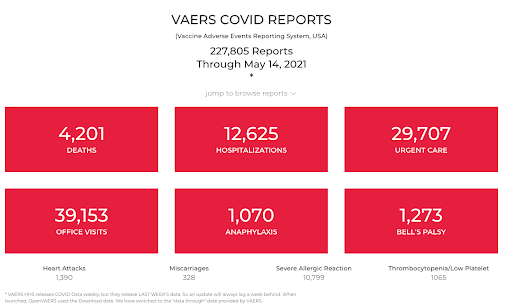
We expect public health authorities to protect us from dangerous products. We were told by public health experts like Dr. Anthony Fauci that this vaccine was “safe and effective.”
But what other product offered to the public has this many reported injuries or deaths without a recall? Something is off with this narrative.
Mysterious Deaths and Injuries After the COVID-19 Shot
After the COVID vaccine was offered to the public, there was a slew of reported deaths in the media, some occurring in celebrities. Over and over again, the media said, “there is no evidence that the COVID vaccine caused these deaths.”
But the apparent question is, “How do they know for sure that the COVID vaccine wasn’t the cause?” The answer is: they do not – there is not enough data to ascertain the full short-term and long-term safety of this vaccine.
Instead, an unfair game is being played with the criterion of the burden of proof by the public health authorities in which the default assumption is that the COVID vaccine was not the cause of death, and they ask the critics or families of the vaccine-injured to “prove it was the vaccine.”
What we do know about is that people are dying after having taken the COVID vaccine. There have been a series of celebrity deaths:
- Rapper DMX experienced a massive heart attack and subsequently died after taking the COVID vaccine.
- Baseball great Hank Aaron passed away three weeks after receipt of the COVID vaccine.
- The same with boxer Marvin Hagler who died after receiving the vaccine.
- Former Detroit news anchor Karen Hudson-Samuels died one day after receiving the COVID vaccine.
- 30-year old actress Ashley Taylor Gerren passed away after receiving it too.
There are plenty of normal people who died after receiving the COVID vaccine. Many of these people just wanted to “get back to normal,” and unfortunately, they will never have this chance:
- Haley Link Brinkmeyer, a 28-year old physical therapist, died two days after taking the COVID vaccine.
- 55-year old Augusta Turiaco fell into a coma and died two days after receiving the COVID vaccine.
- A healthy 35-year old woman Anne VanGeest came down with a terrible headache eight days after receiving the COVID vaccine and died three days later of a brain hemorrhage.
- A 70-year old New York man passed away just 25 minutes after receiving his COVID vaccine.
- A healthy Miami doctor died two weeks after getting the vaccine due to internal bleeding.
- A California resident died several hours after taking the COVID vaccine.
- There are many more death reports from VAERS.
There are many media reports of COVID vaccine injury:
- 17-year old teen hospitalized with blood clots after receiving the COVID vaccine.
- In Kalamazoo, Michigan, a school had to close after multiple teachers had to call out sick after experiencing negative effects of the COVID vaccine.
- Healthcare worker Chavonya Littlejohn suffered a severe allergic reaction to the COVID vaccine and had to be hooked up to a ventilator.
- Nurse researcher Kristen Choi, a participant in the Phase III vaccine trial, after receipt of the COVID vaccine, experienced an extremely high fever of 104.9 °F.
- Many people are reporting “COVID vaccine headaches” that can last up to four days which can be a sign of blood clots in the brain.
- Many women report “heavier and more painful periods” since getting the COVID-19 vaccine.
- Social media has exploded with accounts of vaccine injury (here, here, and here).
The number of actual vaccine injuries experienced by the public is likely under-diagnosed by at least a factor of 10x higher. Most people and their doctors are unaware of vaccine injury and even file a vaccine injury report in VAERS.
All of these deaths should teach us a lesson – rushing a COVID vaccine is “colossally stupid.”
But Are Reports of Injury Causally Related to the COVID Vaccine?
A common criticism of VAERS injury reports is that they are self-reported and cannot be used to establish causality. But such criticism is often used by medical authorities to make the foolish assumption that “reported adverse events are never related to vaccination.”
At best, this is an abuse of the precautionary principle (a principle that suggests in the face of unknowns we should err towards protecting the individual from the new treatment) which protects public health’s vaccine program from criticism. At worst, this is gaslighting reminiscent of the #MeToo movement – powerful authorities do their best to convince the injured recipient that their complaints are all in their heads.
But what the authorities fail to acknowledge is VAERS reports offer valuable signals that something could be wrong with a vaccine. Ignoring such signals can be dangerous such as what happened with the Dengvaxia scandal in the Philippines in which 600 deaths in children were linked to a failed dengue vaccine which, due to a mechanism known as antibody-dependent enhancement, increased susceptibility to dengue.
Correlation is a valuable signal that causation is possible, and ignoring it or dismissing it without adequate investigation is a red flag. It becomes more important to investigate when the number of VAERS reports is abnormally large relative to the other vaccines. Unfortunately, lack of investigation seems to be the norm when it comes to vaccine injury.
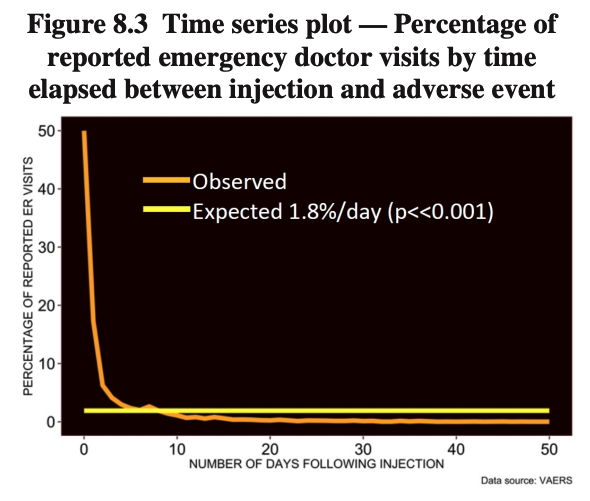
An exciting new paper from the journal Science, Public Health Policy & the Law makes a case for causality for the COVID vaccine and negative adverse events based on a startling intuition – If these adverse events were unrelated to vaccination, then we would expect the probability of reports to be more uniform post-receipt of the COVID vaccine.
However, they aren’t. There are a suspiciously high number of serious events, including emergency room visits and deaths, clustering in the few days right after receipt of the COVID vaccine.
The following graphic from the study shows the clustering probability for ER visits right after the COVID vaccine:
The following graphic from the study shows the clustering probability for deaths right after the COVID vaccine:
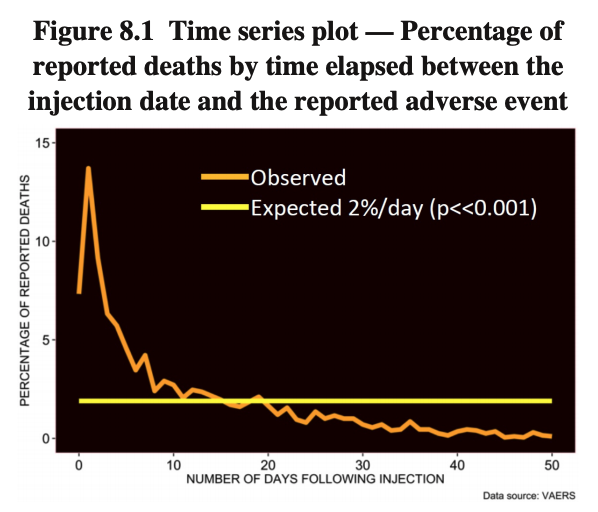
The paper concludes: “Analysis suggests that the vaccines are likely the cause of reported deaths, spontaneous abortions and anaphylactic reactions in addition to cardiovascular, neurological and immunological AEs.”
Editor Dr. James Lyons-Weiler explained the significance of this study: “This study will be hotly debated because it drives to the core presumption that the VAERS data resource cannot be used to assess causality. Temporal association is a critical piece of evidence in causality; the test for clustering of the events so near the vaccination event provides a critical test of the hypothesis of causality.”
This data calls into question the public health authorities’ safety methodology. Shouldn’t the authorities have done a more detailed safety assessment before the widespread dissemination of the COVID vaccine to the public? Do the public health authorities even fully understand the mechanisms of harm from the COVID vaccine?
Unacknowledged Biological Mechanisms for COVID Vaccine Harm
Concurrent with vaccine injury reports, there is new research and testimony from experts regarding the biological mechanism for harm from the COVID vaccine. Arguably these mechanisms should be known by the public before the dissemination of the COVID vaccine.
An important question is, “Why are we vaccinating individuals who are known to have had and recovered from COVID?” There is good research to suggest that COVID immunity is long-lasting.
With 10-20% of the populace having already been exposed to COVID, an important consideration is whether or not we are exposing already-immune individuals to increased risk by giving them the COVID vaccine. If you have had COVID before, some of the virus materials could still be present in your body’s organs, and subsequent receipt of the COVID vaccine could cause your immune system to go haywire.
Pro-vaccine surgeon and researcher Dr. Hooman Noorchashm warns:
“I state the above, because I know, as a matter of scientific principle, that once a person is naturally infected by a virus (any virus), antigens from that virus persist in the body for very long after viral replication has stopped and clinical signs of infection have resolved. So, when a vaccine reactivates an immune response in such recently infected persons, the tissues harboring the persisting viral antigen are targeted, inflamed and damaged by the immune response.
In the case of SARS-CoV-2, we know that the virus naturally infects the heart, the inner lining of blood vessels, the lungs, and the brain. So, these are likely to be some of the critical organs that will contain persistent viral antigens in the recently infected — AND, following reactivation of the immune system by a vaccine, these tissues can be expected to be targeted and damaged.
If young and otherwise healthy persons, recently infected, could tolerate such adverse side-effects of the vaccine, it is highly likely that many of the elderly and frail, or those with serious cardiovascular risk factors, would not.”
The autoimmune disease risk is seldom acknowledged by the media and by the public health authorities. Yet even in those that have not yet gotten COVID-19, there is the risk of autoimmune disease. This paper found that, due to similarity to the spike protein, SaRs-CoV-2 antibodies can cross-react with human tissues (a phenomenon known as molecular mimicry).
The autoimmune has been corroborated by reports from VAERS and the vaccine trials. There have been cases of heart inflammation (myocarditis), Guillain–Barré Syndrome, and Bell’s Palsy in COVID vaccine recipients.
Research suggests too that the spike protein itself can cause damage and unintended consequences to the body. This paper found that the SaRs-Cov-2 spike protein generated from the vaccine can cause abnormal cell signaling and lead to unknown long-term consequences.
The research paper warns: “it is important to consider the possibility that the SARS-CoV-2 spike protein produced by the new COVID-19 vaccines triggers cell signaling events that promote PAH, other cardiovascular complications, and/or complications in other tissues/organs in certain individuals. We will need to carefully monitor the long-term consequences of COVID-19 vaccines that introduce the spike protein into the human body.”
A different research paper found that the spike protein alone can cause lung damage. The presence of the spike protein in the lungs was sufficient to induce damaging inflammation in the lungs of mice.
Another paper postulated that the Pfizer COVID vaccine could raise the risk of prion disease in humans leading to neurological diseases including Alzheimer’s disease and ALS. The research found that certain factors in the vaccine could interfere with proper protein folding or elevated intracellular zinc levels folding, thus leading to neurodegeneration.
Researcher Stephanie Seneff, in a recent interview and paper, expounded on how these mechanisms could work: “Researchers have shown that mRNA vaccines, in contrast with recombinant protein vaccines, elicit a robust development of neutralizing antibodies at these germinal centers in the spleen. However, this also means that mRNA vaccines induce an ideal situation for prion formation from the spike protein, and its transport via exosomes along the vagus nerve to the brain.”
Finally, while the media vehemently asserts that the COVID vaccine cannot alter DNA. It is well-established that 8% of our genome comes from viral DNA. This viral DNA must have gotten here somehow, and the key lies in an enzyme called reverse transcriptase that triggers cells to generate DNA from RNA.
It turns out we already have reverse transcriptase in the body, and this fact makes it wholly possible that mRNA spike protein can integrate into our genome.
Senoff explains it this way: “We actually have plenty of reverse transcriptase in our own cells. We have plenty of it. And it’s these long interspersed nuclear elements (LINEs) and short interspersed nuclear elements (SINEs) that are able to take our RNA back to DNA and to put that DNA back into the genome.”
All of the discussed mechanisms mean something important – the public is not being told the full story regarding the full risks of taking the COVID vaccine.
So What Does COVID Vaccine Injury & Death Mean?
In the face of Covid vaccine mania, we have to consider the implications of what the COVID vaccine means for all of us. Beyond the apparent people who have been hurt or killed by the COVID vaccine, the topic of COVID vaccine injury raises many questions for consideration in our society.
First, there is the question of vaccine transparency. Critical to whether or not to take the vaccine is having all of the available data. For the recipient who ultimately bears the risk, full transparency and informed consent should be the norm. It is clear from this discussion that we do not have this transparency from our national vaccine programs.
Second, our public health and medical institutions need to do some soul-searching regarding how they have dealt with vaccine injury and death. Vaccine injury and death is an inconvenient truth to a long-held paradigm on how to control infectious diseases.
With so many injuries and deaths from the COVID vaccine, the topic of vaccine injury has hit mainstream discussion. It brings attention to public health’s track record of vaccine injury and death denial and the protection of vaccine manufacturers from liability.
Third, the reality of COVID vaccine injury and death calls into question all of the incentives and coercive mechanisms (including vaccine passports and mandates) used to increase vaccine uptake from a moral standpoint. Pretending COVID vaccine injury and death does not exist while pushing the vaccine ignores the #MeToo-like violence done by the COVID vaccine.
The core of all of this is that public health has to change. The reality of COVID vaccine injury and death is that public health has become a militaristic, controlling force that embodies the colonial, paternalistic mind.
How can we begin to make changes to public health?
The critical step is to stop participating in it.
It is your choice whether to participate in coercive mechanisms like vaccine passports or vaccine mandates. It is your choice to remain silent or to speak up against oppressive practices. It is your choice whether we put up with the current practices of public health or demand that we change. And ultimately, it is your choice whether or not to take the (dangerous) COVID vaccine.
And this is public health’s greatest fear – that you will learn the truth about the COVID vaccine and then make use of the choice which was always yours.
By Nate Dormal